For a summary of dos and don’ts click here.
We’ve distilled the learning into 12 themes summarised here. Click the links in the table below for more detail.
We have produced a series of podcasts as part of this work, capturing insight from those who have implemented blended roles.
Please find our podcasts here: Podcasts
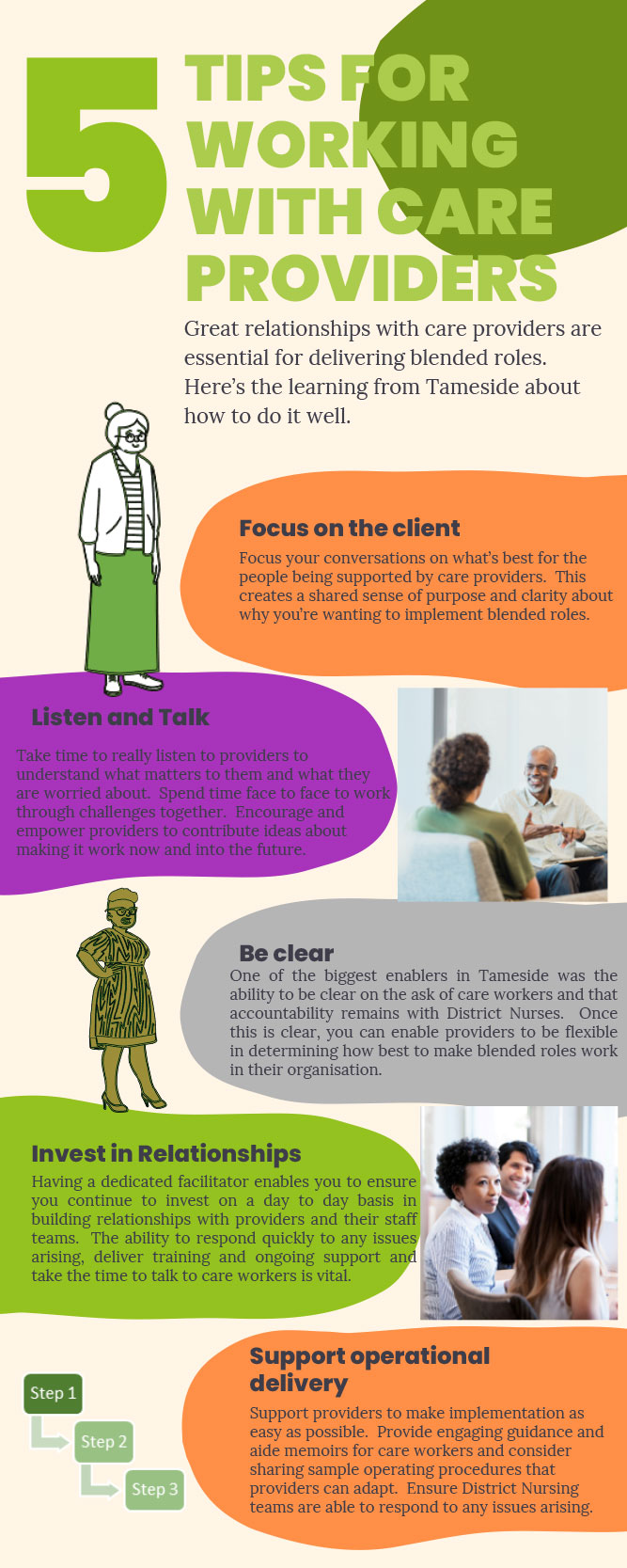
It’s better for residents.
Has to build on strong relationships between carers and district nurses.
Project team (coalition of the willing) relationships crucial.
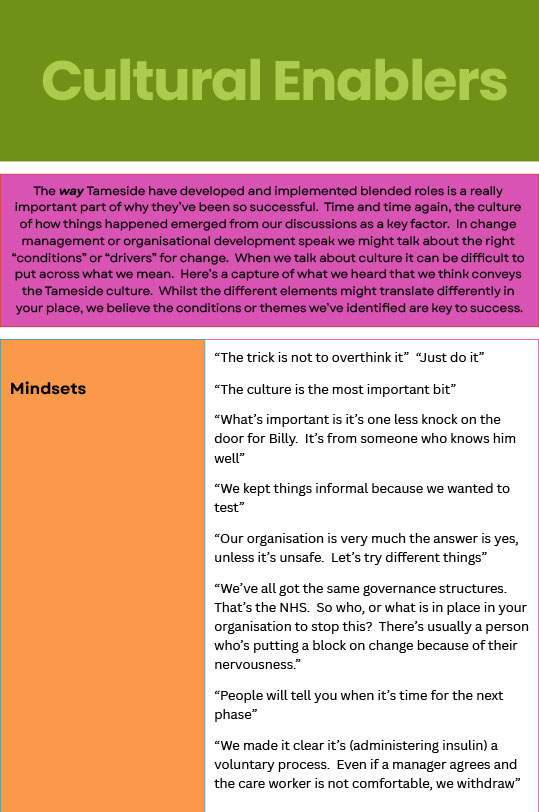
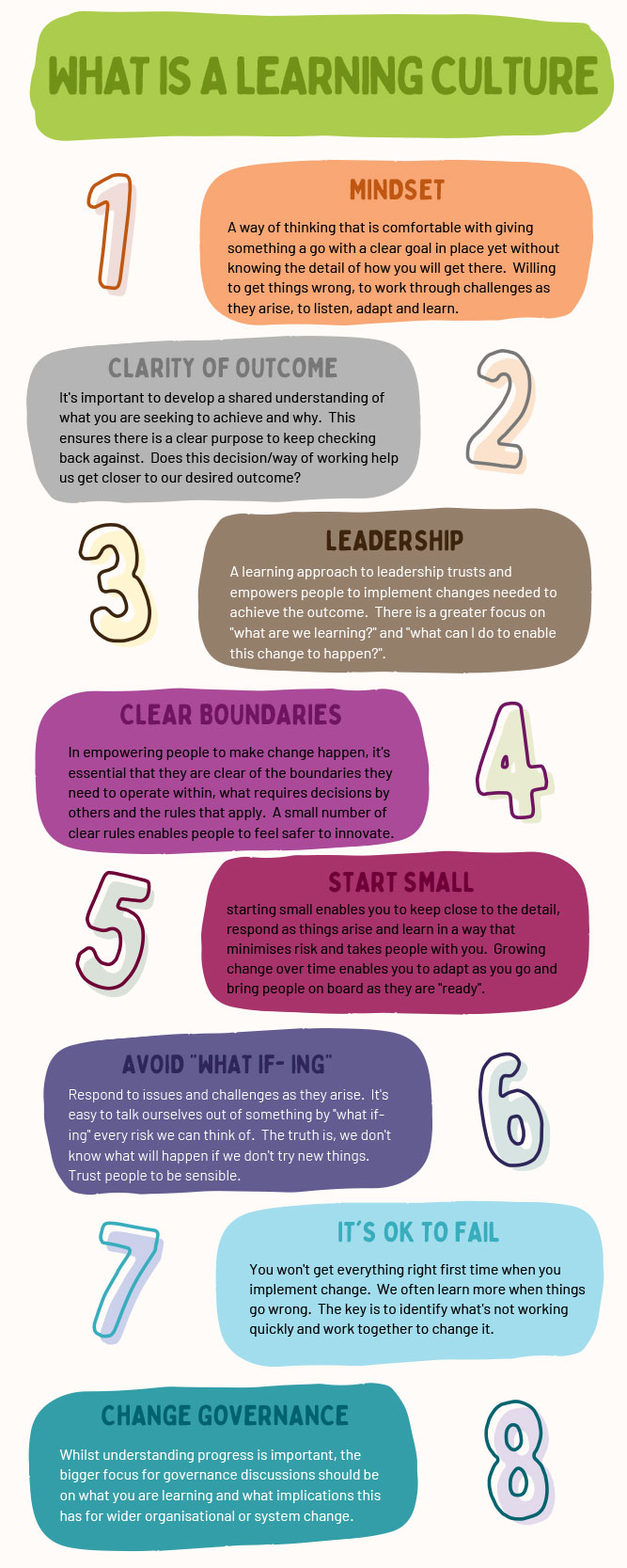
Informal learning approach to leadership grounded in relationships of trust.
- Maturity of integration in Tameside
- Financial uplift to providers
- Took time to evolve
- Built confidence
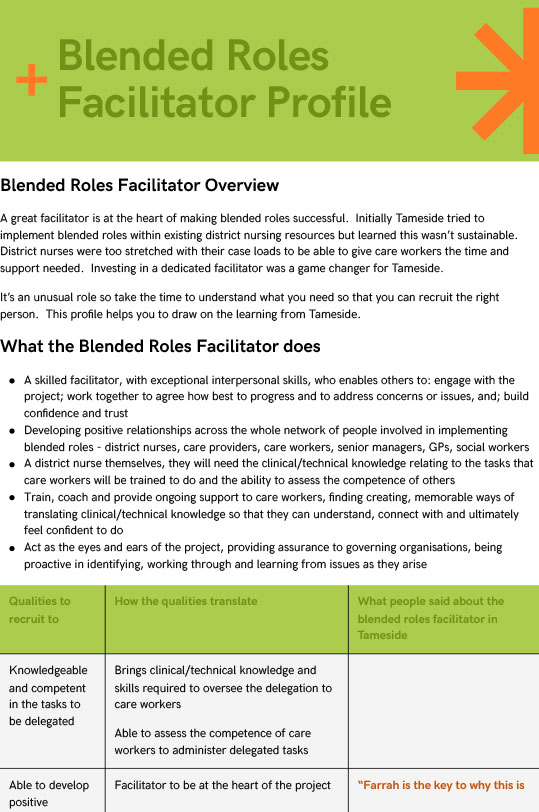
- Blended roles facilitator
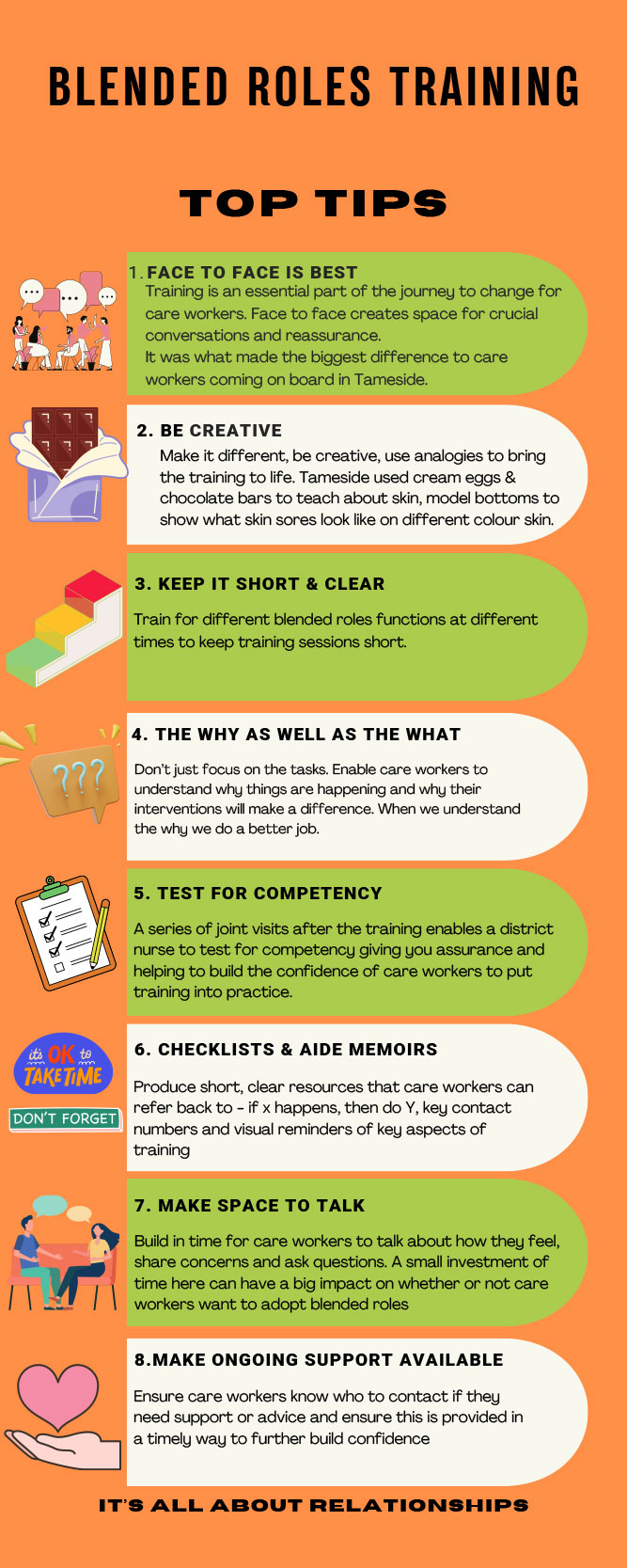
- Face to face, innovative training programme
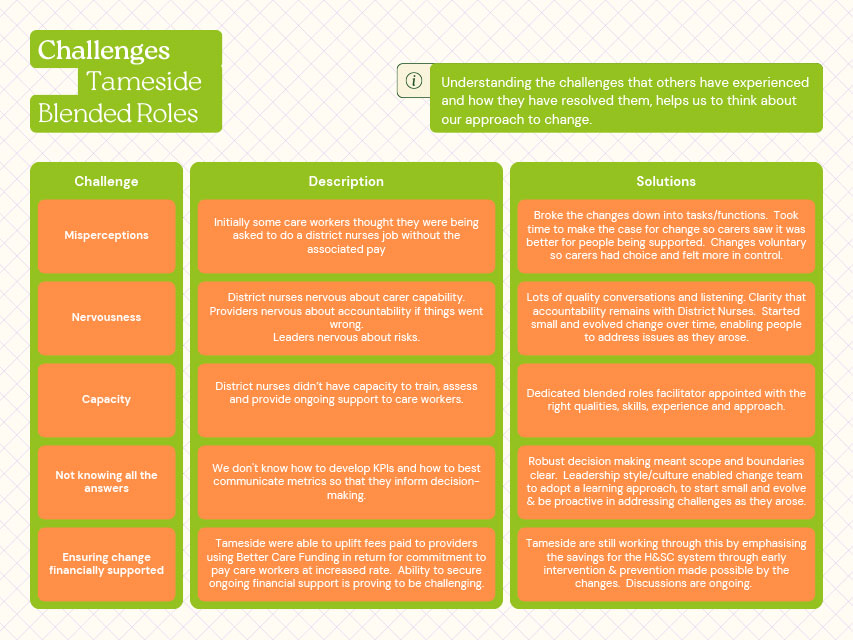
- Initial perceptions from carers of doing job of district nurse
- Nervousness of district nurses
- Nervousness of senior leaders in system
- Financial challenges
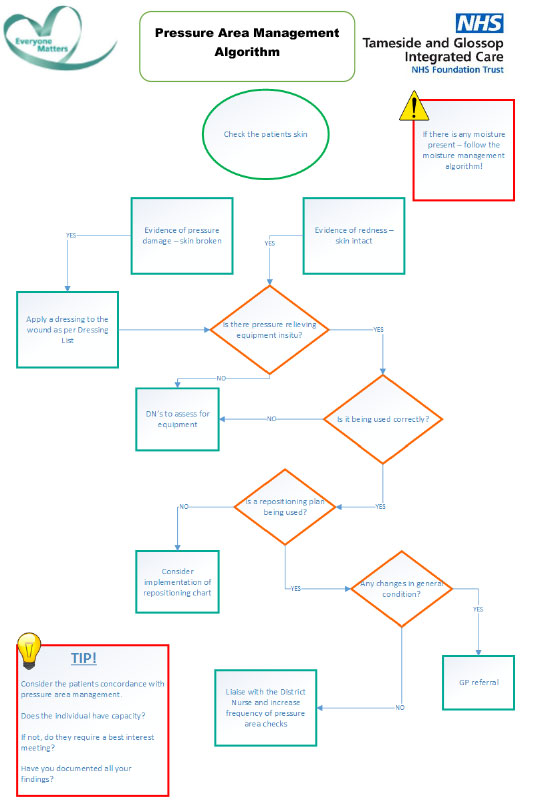
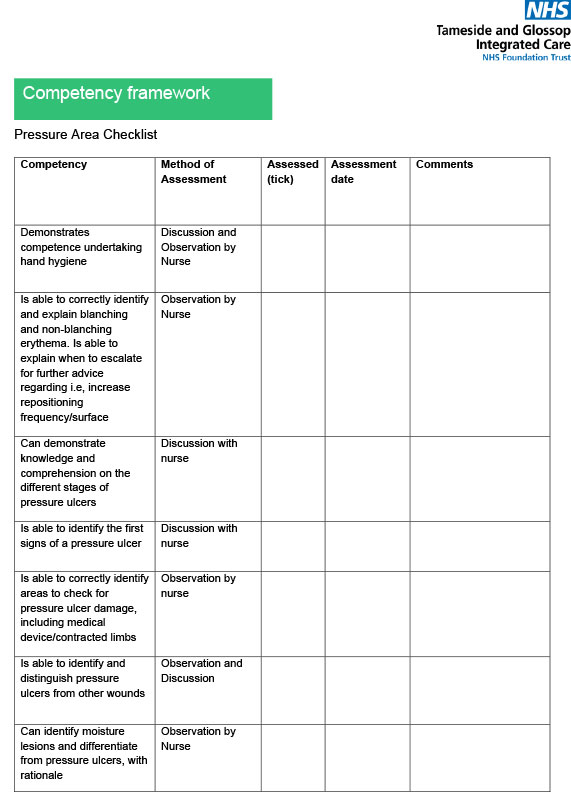
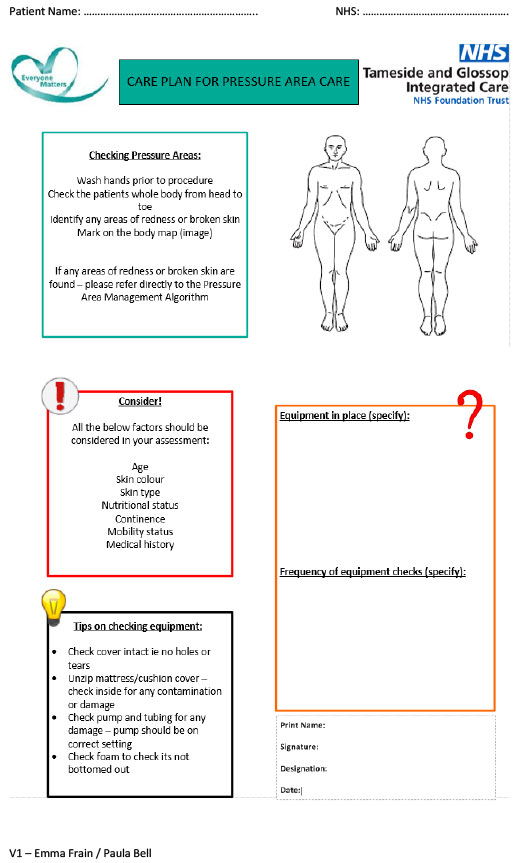
Knowledge, skills & confidence to administer insulin, assess skin health and change dressings underpinned by policy, clarifying who is responsible for what, competency assessments for insulin, pressure areas and wound care, and simple guidance and resources. Small changes, big impact.
- Tight governance
- Learning approach to change management with minimal project mgt
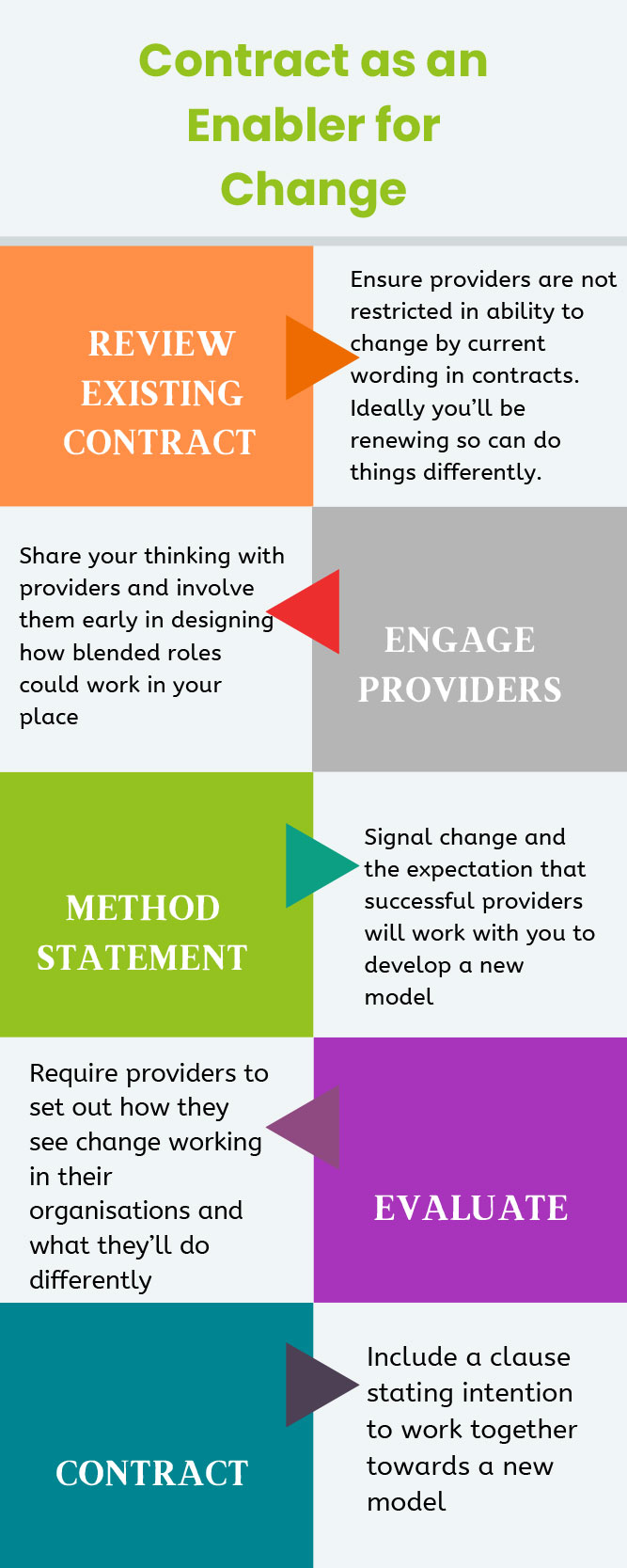
- Developmental contract key
- Initial uplift in fees from joint budgets.
- Clarity about district nurses retaining accountability
- Better for residents/clients.
- Staff feel more knowledgeable & trusted
- Enables earlier intervention
- Great relationships
- Helps with staff retention
- It takes time
- Make it voluntary
- A dedicated facilitator with the right qualities
- Face to face training essential
- Small changes with big impact
- Recognition essential
- Maintain pay differential for carers from National Minimum Wage
- “It’s worked perfectly. Could not fault the whole team”
Lots of potential to do more but progress will be impacted unless fees/pay issue resolved